Childhood is often considered a carefree time of learning, exploration, and joy, unencumbered by the stress and demands of adult life. However, research shows that mental health concerns are common in children and, when left unaddressed, can have long-term negative outcomes. Unfortunately, many young people in Wisconsin have extremely limited access to mental health care, leaving these problems undiagnosed and untreated. Despite these challenges, innovative strategies are springing up to meet the needs of children in Wisconsin, providing opportunities for advocacy around the importance of children’s mental health.
Mental health is an important part of a child’s overall health and well-being, greatly influencing cognitive and social development. However, many children experience mental health problems that make it more difficult for them to learn, grow, and succeed. In fact, almost half of children in the United States experience some type of mental health disorder before age 18, and about 1 in 5 children has, or has had, a severe mental health disorder.[1] These disorders and their care take a heavy emotional, cognitive, and financial toll on children and their families, and are associated with poorer long-term outcomes in physical health, education, social relationships, economic success, and many other areas.[2]
Although mental health problems are often seen as “adult” issues, children can also face severe challenges due to mental health issues. The most commonly diagnosed disorder, Attention-Deficit/Hyperactivity Disorder, is characterized by fidgeting, distractibility, and hyperactivity that is often problematic in classrooms, hindering children’s ability to succeed in school. Depression, another prevalent issue, can cause young people to feel disconnected from friends and loved ones, withdraw from social situations, and can even lead to self-harm or suicidal behavior. Anxiety disorders can make children feel so worried and unhappy that they can’t pay attention in class or play with their friends. Children who have Post-Traumatic Stress Disorder may have nightmares that leave them tired and unable to focus or feel threatened when a classmate makes a loud noise. Clearly, mental health problems can greatly affect the lives of children.
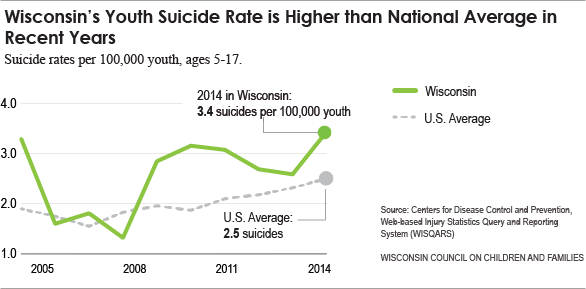
In Wisconsin, concerns over children’s mental health are particularly acute. Wisconsin’s youth suicide rate has been consistently higher than the overall national rate in the last several years, with the rate in 2014 almost 40% higher than the national rate (see Figure 1).[3] The Youth Risk Behavior Survey, a survey given to high schoolers around the state to gather information about what types of behaviors youth engage in, provides more information on the mental health of Wisconsin youth. According to the 2013 report:[4]
- 55.6% of the students who completed the survey reported that their mental health was “not good” at least one of the last 30 days
- 17.3% of youth had purposely hurt themselves, without wanting to die, in the previous 12 months
- 13.2% had seriously considered attempting suicide during the previous 12 months
- 12.1% had made a plan about how to attempt suicide in the previous 12 months
- 6.0% actually attempted suicide at least once in the previous 12 months
- 2.5% made a suicide attempt in the previous 12 months that resulted in an injury, poisoning, or overdose that had to be treated by a doctor or nurse
These statistics are startling and concerning. In the 2014-2015 school year, there were more than 260,000 high school students in Wisconsin. Applying the previous rates to that population suggests that over 15,000 high school students across Wisconsin attempted suicide, and these attempts resulted in injury for more than 5,000 youth. These numbers demonstrate just how devastating mental health issues can be for youth all over Wisconsin. The actual completed suicide rates for children ages five to seventeen are illustrated in Figure 1.
Self-reported poor mental health in Wisconsin is reflected in data comparing youth mental health across states. According to a report by Mental Health America, Wisconsin ranked 44th in the nation for youth mental health, demonstrating both high rates of mental illness and low access to care.[5] Additionally, 11.4% of Wisconsin youth experienced a major depressive episode in the last year—the third worst rate in the nation. For severe major depressive episodes, which seriously interfere with a young person’s school, home, and social functioning, the data is even grimmer. Over 10% of youth had experienced a severe major depressive episode in the previous year—an increase of 6.4% since 2010. This means that in 2014, Wisconsin had more than twice the amount of severely depressed youth than states with the lowest rates (see Figure 2).
Every day, children in every classroom, playground, and community across Wisconsin experience mental health problems and their effects. If left unaddressed, these problems can follow children into adulthood, affecting their social, educational, and economic well-being in the long-term. Because of this, it is vital that children receive appropriate, effective, and high-quality mental health care. Unfortunately, many children in Wisconsin face significant barriers to services that support them on their path to success.
Mental Health Care: Treatment and Services
Given the prevalence, severity, and long-term consequences of mental health problems in children, it is especially important that children have access to effective, high-quality mental health care. However, about one third of all children who needed mental health care in 2012 went without treatment.[6] In Wisconsin, almost 69% of adolescents who experienced a major depressive episode did not receive treatment in the previous year (see Figure 3).[7] Children of color, children without insurance, foreign-born children, and children who do not speak English face even greater barriers to treatment, and often receive fewer and poorer services.[8] For those who do get treatment, receipt of services often takes a great deal of time and places additional financial and practical burdens on families. Although many chronic mental illnesses begin in childhood and adolescence, an average of 8-10 years passes between onset of symptoms and intervention, all too often allowing mental health problems to continue unabated.[9] Despite the need, children in Wisconsin are not getting the mental health care they deserve.
Without services to prevent and treat mental health issues, problems can worsen in frightening ways that have a life-long impact. In school, unaddressed mental health problems can lead to suspensions and expulsions that limit educational opportunities and achievement. Youth who have externalizing symptoms of mental health problems, such as aggression and delinquency, may become involved in the juvenile or criminal justice systems, which are more punitive and less rehabilitative than traditional mental health care settings. In extreme cases, confused and frustrated caregivers may feel the only option for children with severe mental health issues is psychiatric hospitalization, which is short-term, expensive, and often traumatic for children. The most devastating result of unmet mental health needs is suicide, which can irreparably harm families, schools, and communities. Unfortunately many children with mental health problems in Wisconsin are pushed down these difficult paths because of barriers to treatment related to geographic and workforce limitations.
Geographic and Workforce Limitations in Mental Health Care
Children all over Wisconsin need mental health care, but many face significant barriers based on where their families live. Nationally, more than three-quarters of counties have a severe shortage of psychiatrists and other mental health professionals, with particularly acute shortages in rural areas and counties with lower per capita incomes.[10] The same pattern exists in Wisconsin, limiting access to appropriate mental health care for children, especially in less-populated areas.
As of 2013, forty-four counties, plus some additional areas in Wisconsin, were designated by the federal government as Health Professional Shortage Areas (HPSAs) for mental health services.[11] HPSAs have lower-than-desired ratios of psychiatrists compared to the general population, may have unusually high needs for services, and do not have access to resources in nearby areas. For highly-trained and educated mental health professionals, like psychiatrists and psychologists, the shortage is even greater. Only four counties in Wisconsin did not have some level of unmet need for psychiatrists, and sixteen counties had no psychiatrists at all.[12] Statewide, Wisconsin had fewer than 1000 active psychologists in 2013, less than half the number of our neighbor, Minnesota.[13]
These shortages are problematic for anyone in need of mental health services, but particularly so for children. Because of the unique joys and challenges of childhood, children should receive mental health care from individuals who have specific training and experience working with young people. Child and Adolescent Psychiatrists (CAPs) who can provide medical expertise and prescribe medication are especially important in providing mental health care for children. Unfortunately, the workforce of child-focused mental health professionals is also extremely limited, with most counties in Wisconsin lacking even one Child and Adolescent Psychiatrist, and none having a sufficient supply (see Figure 4).[14] This pervasive absence of child-focused mental health professionals leads to long wait times for services while mental health problems stagnate or perhaps worsen. Alternatively, some children receive care from psychiatrists who lack vital child-specific expertise, which may be ineffective or even harmful.
Many children in Wisconsin do not receive mental health care that supports their well-being and long-term success. Unfortunately, barriers to treatment are pervasive system-wide issues that are extremely difficult to change. Even so, some innovative programs and practices have arisen to better meet the mental health needs of Wisconsin’s youth.
Strategies for Increasing Access to Children’s Mental Health Care
Despite persistent and pervasive barriers to accessibility for children to receive mental health care, communities and professionals across Wisconsin have undertaken innovative strategies to meet the needs of children. These strategies leverage and expand the reach of existing resources to ensure that all children have access to mental health care. The following programs demonstrate promising approaches to gaps in children’s mental health care in Wisconsin.
Trained and Supported Pediatricians: Child Psychiatry Consultation Program (CPCP)
Widespread shortages of mental health professionals, especially Child and Adolescent Psychiatrists, often shift the burden of mental health care to primary care doctors, who are more accessible to many children and families. However, these physicians often do not have training specifically related to mental health concerns, limiting their effectiveness. The Child Psychiatry Consultation Program ameliorates this problem by providing support for primary care physicians in addressing children’s mental health concerns. Through CPCP, mental health professionals can connect with primary care doctors to provide case consultation and guidance in diagnosing and managing mild to moderate mental health problems in children. Participating physicians also receive education and training in children’s mental health to augment their own skills. Finally, CPCP disseminates information about regional mental health resources through primary care physicians, better connecting children and their families with needed resources.
Started in 2012 with generous philanthropic support from Dr. Michael and Mrs. Billie Kubly through the Medical College of Wisconsin, the program originally provided mental health consultation services to physicians in the Milwaukee metropolitan area.[15] Due to the program’s success, the state of Wisconsin passed legislation in 2013 to provide an additional $1 million to expand services. CPCP now also serves sixteen counties in northern Wisconsin, where mental health resources are especially scarce. Initial data since the expansion has shown positive results, with over 120 physicians enrolled in the Northern region and more than 140 in the Milwaukee area.[16] Encounters between primary care physicians and mental health professionals are primarily related to medication and diagnostic questions, and physicians received a response time within 30 minutes in the vast majority of cases. Due to its success, many hope that the CPCP will soon be expanded to serve primary care physicians statewide. For children with mental health needs and for their primary care doctors, CPCP is an innovative way to ensure that patients receive appropriate treatment, even in areas with limited mental health resources.
For more information on the Wisconsin Child Psychiatry Consultation Program, visit www.chw.org/cpcp.
Mental Health Care from a Distance: Tele-Mental Health
Another approach to addressing mental health provider scarcity is through telehealth programs, which provide “patient care at a distance” when providers are not accessible in person. This is achieved through the use of high-quality, interactive technologies that connect providers and patients in ways that are functionally similar to in-person meetings. Although telehealth is used for many types of health care, it is growing especially rapidly in the field of mental health as a response to widespread provider shortages, especially in rural areas. Tele-mental health services can include consultation, assessments, medication management, and counseling between a patient and a distant provider, and can occur with greater ease and frequency than in-person appointments.[17] In areas where mental health professionals are not easily accessible, tele-mental health also tends to be less expensive than traditional mental health care, as it does not require additional travel and recruitment expenses. Access to mental health care is extremely important, and evidence shows that the benefits of ongoing, quality care from a mental health professional can occur even when it is not provided in person.
In 2013, the Wisconsin state legislature passed Act 130, which allowed for the provision of mental health services via high-quality, technology-based mediums to be reimbursable through Medicaid, as long as providers met certain standards related to licensure and certification. Tele-mental health services are also covered by many private insurance plans and, as it gains popularity and credibility as an alternative to traditional mental health care, many hope that coverage will expand. Given the lack of child-specific mental health professionals all over Wisconsin, tele-mental health allows children with mental health needs to receive care to which could not otherwise access.
For more information on tele-mental health in Wisconsin, read the Department of Health Services report on the subject at https://www.dhs.wisconsin.gov/dqa/memos/15-011.pdf.
School-Based Mental Health: United Way’s PATH for Students
In addition to provider-related challenges, children often experience practical barriers to mental health care, such as transportation and insurance. To eliminate these barriers, many school districts in Wisconsin have begun to provide mental health care in schools. One such program, PATH (Providing Access to Healing) for Students, is a partnership between the United Way Fox Cities, nearby school districts, and area mental health providers. The program offers mental health care to elementary, middle, and high school students who experience barriers to community care, such as limited financial resources, transportation issues, waiting lists, lack of parental support, and language barriers. School-based programs such as PATH circumvent these barriers by providing mental health care directly in schools, where children spend less time away from the classroom and do not need parents to transport them. Students also tend to feel more comfortable in school than in other traditional mental health care settings, and are thus more open to services and more likely to self-refer or refer friends. Because school-based services are delivered via the school district, students receive care regardless of their ability to pay, making it an effective option for uninsured or under-insured families.
United Way’s PATH for Students began as a pilot program in one school district in 2008, but expanded in 2011 to ten more school districts. PATH has served over 1000 children and adolescents since its inception and has shown extremely positive results.[18] Sixty-nine percent of students reported experiencing reduced symptoms and increased functioning, and nearly two-thirds of students showed improved academic performance and school behaviors. Almost all of the students said they would return to therapy if needed, demonstrating the positive impact PATH has on students. A cost-benefit analysis by the Robert M. La Follette School of Public Affairs at UW-Madison in 2014 also showed the cost effectiveness of PATH, with net benefits of the program reaching $9,384,000 (more than $50,000 per student) through avoided medical costs, increased productivity and quality of life, and decreased suicide risks. Participating school districts also felt the financial benefits of the program, with fewer expenses related to truancy, behavioral problems, and counseling. School-based mental health programs like PATH demonstrate the importance of overcoming barriers and providing needed mental health care for children, at the great benefit of all involved.
For more information on United Way’s PATH for Students, visit https://www.unitedwayfoxcities.org/our-work/united-ways-path-for-students/
The Wisconsin Department of Public Instruction (DPI) has also recognized the importance and benefits of school-based mental health services. As such, DPI has developed the Wisconsin School Mental Health Framework, which uses multi-level systems to provide varying levels of support for students in Wisconsin schools. The Framework calls for school wide practices that promote social-emotional development, healthy relationships, and individual well-being for all students. It also includes more focused interventions, such as individualized wellness plans and collaboration with family members for some students who demonstrate additional needs. Finally, for students who are experiencing high mental needs or concerns, the Framework calls for targeted interventions like counseling, referral to other resources, and safety planning. This tiered system allows for all students to receive support related to mental health issues while also providing additional resources for those who need them. The following programs are among the strategies described by the Wisconsin School Mental Health Framework:
- Trauma-Sensitive Schools
- Safe Schools, Healthy Students Project
- Youth Mental Health First Aid
- SBIRT (Screening, Brief Intervention, Referral to Treatment)
- The PREPaRE Training Curriculum
To read about the Wisconsin School Mental Health Framework and learn about examples of school-based mental health services in communities across Wisconsin, visit http://dpi.wi.gov/sites/default/files/imce/sspw/pdf/mhframework.pdf.
For more general information about school-based mental health services through the Department of Public Instruction, visit http://dpi.wi.gov/sspw/mental-health.
It’s Not Rocket Science – There are Things We Can Do To Make Our Children’s Lives Better
The previously discussed strategies are important and innovative ways to help meet the mental health needs of youth. However, each of these programs requires a great deal of resources and support to ensure they are successful. As such, we advocate for:
- Expansion of the Child Psychiatry Consultation Program
Initial investments in CPCP have demonstrated great outcomes, but benefits are limited to those in the selected pilot program areas. Children all over Wisconsin need mental health care and, if primary care physicians are providing it, they need education, training, and support.
- Mandatory Coverage for Tele-Mental Health by Private Insurers
Wisconsin Act 130, which mandated that certified tele-mental health services be covered by medical assistance, was a vital step toward the provision of mental health care at a distance. However, private insurers may still choose not to cover these services, adding barriers that may keep children from accessing mental health care. Mandated parity of tele-mental health services to traditional mental health care would support access for families with private insurance.
- Support for School-Based Mental Health Efforts
The Wisconsin Department of Public Instruction has recently developed the Wisconsin School Mental Health Framework[19], which promotes and facilitates school-based mental health efforts across the state. It is vital that school districts adopt the framework to identify the mental health needs of their students and work toward meeting them. Additionally, statewide and district-specific investments in school-based mental health programs will be necessary to provide necessary resources.
- Incentives for Mental Health Providers in Shortage Areas
Given the widespread shortages of mental health professionals, especially those with expertise in treating children, incentives for individuals to receive training in child psychiatry and/or practice in underserved areas are important for workforce health. In 2014, Governor Scott Walker signed Act 128, which provided grant opportunities for twelve Wisconsin-trained psychiatrists who practice in an underserved region in the state. Act 128 is a great foundation for grant-based incentives for mental health providers, but there is room for expansion in order to include more psychiatrists, especially those who treat children and adolescents. Other incentives, such as tax- and income-based incentives, may also be helpful in strengthening the mental health workforce in Wisconsin.
- Continued Monitoring of Children’s Mental Health in Wisconsin
In 2013, the Office of Children’s Mental Health (OCMH) was created as an overarching agency concerned with children’s mental health in Wisconsin, focused on improving access to services, facilitating communication between child-serving agencies, coordinating initiatives, and tracking program performance related to children’s mental health. The OCMH also provides annual reports to the legislature on its efforts to innovate, integrate, and improve children’s mental health. The work of the OCMH is extremely important for progress monitoring and ensuring that children’s mental health remains a priority in Wisconsin.
Summary
Mental health issues affect children all over Wisconsin, hindering their potential in concerning ways. Sadly, many of these children do not receive the care they need due to circumstances outside of their control. When Wisconsin fails to meet the mental health needs of its youngest citizens, children and their families suffer and communities feel the impacts of lost potential. Fortunately, there are effective strategies for ensuring that all children have access to mental health care that supports them on a path toward lifelong success. It is vital that individuals, groups, and stakeholders advocate for the support and expansion of efforts that connect children in Wisconsin to the mental health care they need and deserve.
[1] Merikangas, K. R., He, J., Burstein, M., Swanson, S. A, Avenevoli, S., Cui, L., Benjet, C., Georgiades, K., Swendsen, J. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Study-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980-989.
[2] Alegría, M., Greif Green, J., McLauglin, K. A., & Loder, S. (2015). Disparities in child and adolescent mental health and mental health services in the U.S. William T. Grant Foundation. Retrieved from http://wtgrantfoundation.org/library/uploads/2015/09/Disparities-in-Child-and-Adolescent-Mental-Health.pdf.
[3] Centers for Disease Control. Fatal Injury Reports, 1999-2014, for National, Regional, and States. Retrieved from http://www.cdc.gov/injury/wisqars/.
[4] Wisconsin Department of Public Instruction. (2013). Youth Risk Behavior Survey results. Retrieved from http://dpi.wi.gov/sspw/yrbs.
[5] Mental Health America. (2016). The state of mental health in America. Retrieved from http://www.mentalhealthamerica.net/sites/default/files/2016%20MH%20in%20America%20FINAL.pdf.
[6] Office of Children’s Mental Health. (2014). Report to the Wisconsin Legislature. Retrieved from http://dpi.wi.gov/sites/default/files/imce/sspw/pdf/mhchildrensmentalhealthreport2014.pdf.
[7] Mental Health America. (2016). The state of mental health in America. Retrieved from http://www.mentalhealthamerica.net/sites/default/files/2016%20MH%20in%20America%20FINAL.pdf.
[8] Alegría, M., Greif Green, J., McLauglin, K. A., & Loder, S. (2015). Disparities in child and adolescent mental health and mental health services in the U.S. William T. Grant Foundation. Retrieved from http://wtgrantfoundation.org/library/uploads/2015/09/Disparities-in-Child-and-Adolescent-Mental-Health.pdf.
[9] American Academy of Child and Adolescent Psychiatry. (2013, May). Child and Adolescent Psychiatry workforce crisis: Solutions to improve early intervention and access to care. Retrieved from https://www.aacap.org/App_Themes/AACAP/docs/Advocacy/policy_resources/cap_workforce_crisis_201305.pdf.
[10] Wisconsin Department of Health Services, Division of Mental Health and Substance Abuse Services. (2014, February). Wisconsin mental health and substance abuse needs assessment (Report No. P-00613). Retrieved from
https://www.dhs.wisconsin.gov/publications/p0/p00613.pdf.
[11] Wisconsin Department of Health Services, Division of Public Health. (2013, June). Wisconsin mental health HPSAs (Report No. P-00515A). Retrieved from https://www.dhs.wisconsin.gov/publications/p0/p00515a.pdf.
[12] Wisconsin Department of Health Services, Division of Mental Health and Substance Abuse Services. (2014, February). Wisconsin mental health and substance abuse needs assessment (Report No. P-00613). Retrieved from
https://www.dhs.wisconsin.gov/publications/p0/p00613.pdf. page 48
[13] American Psychological Association (2015). Demographics of the U.S. psychology workforce: Findings from the American Community Survey. Washington, DC: Author.
[14] American Academy of Child and Adolescent Psychiatry. (2015). Workforce maps by state. Retrieved from http://www.aacap.org/aacap/Advocacy/Federal_and_State_Initiatives/Workforce_Maps/Home.aspx.
[15] Children’s Hospital of Wisconsin. (2016). Child Psychiatry Consultation Program (CPCP). Retrieved from www.chw.org/cpcp.
[16] Children’s Hospital of Wisconsin. (2015). CPCP fact sheet. Retrieved from www.chw.org/cpcp.
[17] Wisconsin Department of Health Services, Division of Quality Assurance. (2015, August). Mental health and substance use telehealth: Criteria for certification. Retrieved from https://www.dhs.wisconsin.gov/dqa/memos/15-011.pdf.
[18] United Way Fox Cities. (2016). United Way’s PATH for Students. Retrieved from https://www.unitedwayfoxcities.org/our-work/united-ways-path-for-students/.
[19] Wisconsin Department of Public Instruction. (2015, December). The Wisconsin School Mental Health Framework: Integrating school mental health with Positive Behavioral Interventions & Supports (Bulletin No. 16050). Retrieved from dpi.wi.gov/sspw/mental-health.
[20] National Association on Mental Illness. (n.d.). LGBTQ. Retrieved from https://www.nami.org/Find-Support/LGBTQ.
[21] Wisconsin Department of Public Instruction. (2013). Wisconsin Youth Risk Behavior Survey: Risk behaviors and sexual identity report. Retrieved from http://dpi.wi.gov/sites/default/files/imce/sspw/pdf/yrbs13hssexualid.pdf
[22] O’Connor, C., Finkbiner, C., & Watson, L. (2012). Adverse Childhood Experiences in Wisconsin: Findings from the 2010 Behavioral Risk Factor Survey. Madison, WI: Wisconsin Children’s Trust Fund and Child Abuse Prevention Fund of Children’s Hospital & Health System.