Communities of color often face greater health challenges that lead to larger health disparities between them and their white peers. This is especially true for the Native American community. Health indicators for Native Americans in Wisconsin are far worse than the health metrics for the state’s white residents. The alarming disparities are deep-rooted and will not be easy to solve, but it’s time to get serious about closing the huge gaps in health and life expectancy in Wisconsin.
One factor in the enormous health disparities is that the federal government has not honored its commitment to provide adequate funding for Indian Health Services (IHS). However, a recent change in federal policy for reimbursing Medicaid costs for Native Americans could significantly increase funding for and accessibility to health services for Native Americans in our state.
Whether the increased funding makes a dent in the extreme disparities in health for Native Americans in Wisconsin will depend on whether state officials, Indian Health Services, and private health care providers work together to close gaps in services and improve care coordination.
Background
Native Americans play an integral role in Wisconsin’s communities, culture, and economy. The state is home to 11 federally recognized tribes and has a Native American population of 86,000. Native Americans reside in urban areas, in rural communities, and on federally recognized Indian reservations throughout Wisconsin. Although many cities, lakes, and rivers in Wisconsin are named after Native Americans, they are often left behind in fights for equity in health care, education, and economic prosperity. Due to the lasting effects of colonization, forced assimilation, and the removal of resources, many native communities suffer from disproportionately high child poverty rates, roadblocks to economic success, and generally low health outcomes.
According to U.S. Census Bureau data, 39.1% of Native American children live in poverty compared to 11.7% of their white counterparts.1 Additionally, just over half the native children in Wisconsin live in households where neither parent has full-time, year-round employment, while around one-fifth of white children face the same circumstance.2 These disparities exist because Native American communities often lack general resources, educational opportunities, and access to family-supporting jobs.
Since the Great Recession, smart investments in infrastructure and social programs have decreased unemployment nationwide, but these investments have often excluded native communities, and native unemployment rates have remained in double digits.3 Chronic joblessness and poverty have also taken a toll on kids trying to complete their education and get ahead. From 2012-2013, 27% of native students did not graduate from high school on time compared with 4% of their white peers.4 These kinds of roadblocks create a cycle of poverty where children are more likely to remain in poverty than escape it.
Large disparities in health indicators for Native Americans
When it comes to health outcomes, the trend in disparities continues:
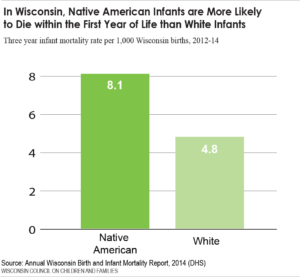
- From 2012-2014, infant mortality rates for native children in Wisconsin were 69% higher than those of white children.5
- The 2014 age-adjusted mortality rate was nearly 50% higher for Native Americans in Wisconsin than for whites (1036 vs. 702 deaths per 100,000 people).6
- The 2014 average age at death for Native Americans was 63 years compared to 77 years for whites.7
- The 2009-2013 average cancer age-adjusted mortality rate was 37% higher for Native Americans in Wisconsin than for whites.8
- The 2014 diabetes mortality rate was almost four times higher for Native Americans in Wisconsin than for whites.9
- Native A
 mericans in Wisconsin also suffer high rates of suicide, especially for children under 18 who have the highest age-adjusted suicide rate (2.5 deaths per 100,000) across all races.10
mericans in Wisconsin also suffer high rates of suicide, especially for children under 18 who have the highest age-adjusted suicide rate (2.5 deaths per 100,000) across all races.10
This data is unsurprising, given the unacceptably low access to health care available to native people. In terms of health insurance, 29.6% of nonelderly native adults in Wisconsin and 15.6% of native children have no insurance, compared with 8.7% of white nonelderly adults and 4.1% of white children who are uninsured.11
New Medicaid Policy Regarding Medicaid Reimbursement for Tribal Healthcare
Earlier in 2016, the Centers for Medicare and Medicaid Services (CMS), released new guidance that could potentially help increase access to health services, improve care coordination for tribal health patients receiving Medicaid services, and provide additional support for IHS providers. It could also yield savings for the state that could be reinvested in improved health services.
Until this year, only facility services rendered within an IHS clinic or tribal health facility for Native American patients with Medicaid have been fully reimbursed by the federal government. Wisconsin’s regular state Medicaid match rate (which is about 42%) applies to the cost of other Medicaid covered services for tribal members that are provided outside of the facility. The new guidance expands the scope of services that qualify for the 100% federal funding to include any Medicaid benefit covered by the state plan that an IHS or Tribal facility is authorized to provide. This may include non-emergency transportation and related travel expenses, home and community based services, and personal care services.
The new guidance also expands the range of providers whose services can qualify for the 100% match to include Urban Indian Health Centers and non-Indian providers. In order for the full federal match rate to extend to services from providers outside of an IHS clinic or tribal health center, the IHS or tribal facility would need to establish a care coordination agreement with the non-IHS/Tribal facilities that they are referring their patient to. In addition, the IHS/Tribal facility would remain responsible for coordinating the patient’s care and retains control of the patient’s medical record.

Implementing this new policy change will not occur overnight. IHS/Tribal clinics along with the state Medicaid programs will need to assess potential changes needed within their current administrative infrastructure to ensure compliance with the increased care coordination responsibilities.
Recent Innovations and Other Policy Proposals
The potential for increased access to care for native people resulting from the new Medicaid guidance regarding full federal reimbursement is only one of the myriad of steps that need to be taken to help support the woefully underfunded Indian Health Services and the native people that it serves. President Obama, in his FY2017 budget included the extension of the 100% federal funding as well as a proposal increasing funds to Indian Health Services to $6.6 billion, a $402 million raise. The increased funds would help expand substance abuse treatment, support the integration of physical and behavioral health, and implement more suicide prevention and domestic violence programs.
This proposal will help tribes broaden access to much needed services and promote recent innovations in improving care for their members.
Innovations in Tribal Health in Wisconsin
Despite these daunting barriers to health and well-being, native communities are making important strides through their own innovative initiatives.
The Bad River Band of Chippewa Indians recently built a state-of-the-art health center on their reservation in Northern Wisconsin as a response to limited access to care for tribal members.12 In addition to being the primary care clinic, the center offers dental and optical services, and prides itself on its comprehensive preventive health measures, early treatment of diabetes, and behavioral health services.
The Menominee Nation has forged a partnership between their local school district and tribal clinic to bring access to dental care, in-class meditation, and other services right into the schools. The initiative has revealed a significant connection between improvements in physical and mental health and academic achievement, as evidenced by their increase in four-year graduation rates from below 60% in 2007 to almost 99% in 2014.
The Waaswaaganing Anishinaabeg Tribe, also known as Lac du Flambeau, established an intergenerational youth empowerment program called ENVISION that uses Ojibwe cultural practices to improve academic performance, redirect at-risk youth, and improve spiritual, emotional, and physical health within the tribe. They have also pioneered restorative housing reserved for those recovering from addiction, as an alternative to incarceration.13
Conclusion
A recent Medicaid policy change, which expands the scope of 100% federal funding for Indian Health Services, offers an exciting opportunity to reduce the huge gap in health and longevity between Native Americans and whites in Wisconsin.
Of course, eliminating the enormous health disparities will require much more than implementation of the recent Medicaid policy change; Wisconsin will also have to alleviate poverty and mitigate other social determinants of health. In the meantime, improving access to quality health services is a very important place to start. If state health officials, Indian Health Services, tribal clinics, and private providers work together to take advantage of the potential increase in federal funding, we can begin to reduce some of the alarming gaps in health care and health outcomes in Wisconsin.
(Endnotes)
1WCCF analysis of 2010-2012 American Community Survey data
2 KIDS COUNT Data Center, “Families without full-time year round employment.” Population Reference Bureau, analysis of data from the U.S. Census Bureau, 2008 – 2014 American Community Survey, http://datacenter.kidscount.org/data/tables/5064-children-living-in-families-where-no-parent-has-full-time-year-round-employment-by-race?loc=51&loct=2#detailed/2/51/false/869,36,868,867,133/10,11,9,12,1,185,13/11486,11487
3 WCCF analysis of 2010-2012 American Community Survey data
4 KIDS COUNT Data Center, “High school students not graduating on time by race and ethnicity.” Population Reference Bureau, analysis of data from the U.S. Department of Education. U.S. Department of Education, National Center for Education Statistics, Common Core of Data (CCD), State Dropout and Completion Data: 2005-2006 through 2012-2013, http://datacenter.kidscount.org/data/tables/7755-high-school-students-not-graduating-on-time-by-race-and-ethnicity?loc=51&loct=2#detailed/2/51/false/1124,1024,937,809,712/12,141,725,4041,1,13/17852,14945
5 Wisconsin Dept. of Health Services, Division of Public Health, Office of Health Informatics. Annual Wisconsin Birth and Infant Mortality Report 2014, https://www.dhs.wisconsin.gov/publications/p01161-15.pdf
6 Wisconsin Dept. of Health Services, Division of Public Health, Office of Health Informatics. Wisconsin Interactive Statistics on Health (WISH) data query system, https://www.dhs.wisconsin.gov/wish/cancer/index.htm.
7 Ibid.
8 Ibid.
9 Ibid.
10 Ibid
11 WCCF analysis of 2010-2014 American Community Survey data
12 Rolo, Marc Anthony. “Something to be thankful for in Indian country” Wisconsin State Journal. Lee Enterprises. 23 Nov. 2015. Web. 4 Apr. 2016.
13 “Robert Wood Johnson Foundation Awards Eight Communities the RWJF Culture of Health Prize” Robert Wood Johnson Foundation. RWJF.org. 28 Oct. 2015. Web. 4 Apr. 2016.